IN A dusty yard in Magagasi, a small village in eastern Swaziland, a man in surgical gloves draws Gugu Dlamini’s blood for the third time this year. The health worker lays a drop of it on a small plastic tray and adds a clear solution. The ritual is familiar. Every time a malaria case is reported in the country, surveillance officers sweep in and test everyone living within 500 metres of the sick person. In a few minutes a single line appears in the tray’s indicator window: Ms Dlamini does not have malaria.
Such vigilance has brought Swaziland to the threshold of becoming the first malaria-free country in sub-Saharan Africa, the part of the world most blighted by the disease (see map). Swaziland’s struggle is part of a wider battle that the world is waging—and winning. If it succeeds, Swaziland will join more than 100 countries that have eliminated malaria within their borders.
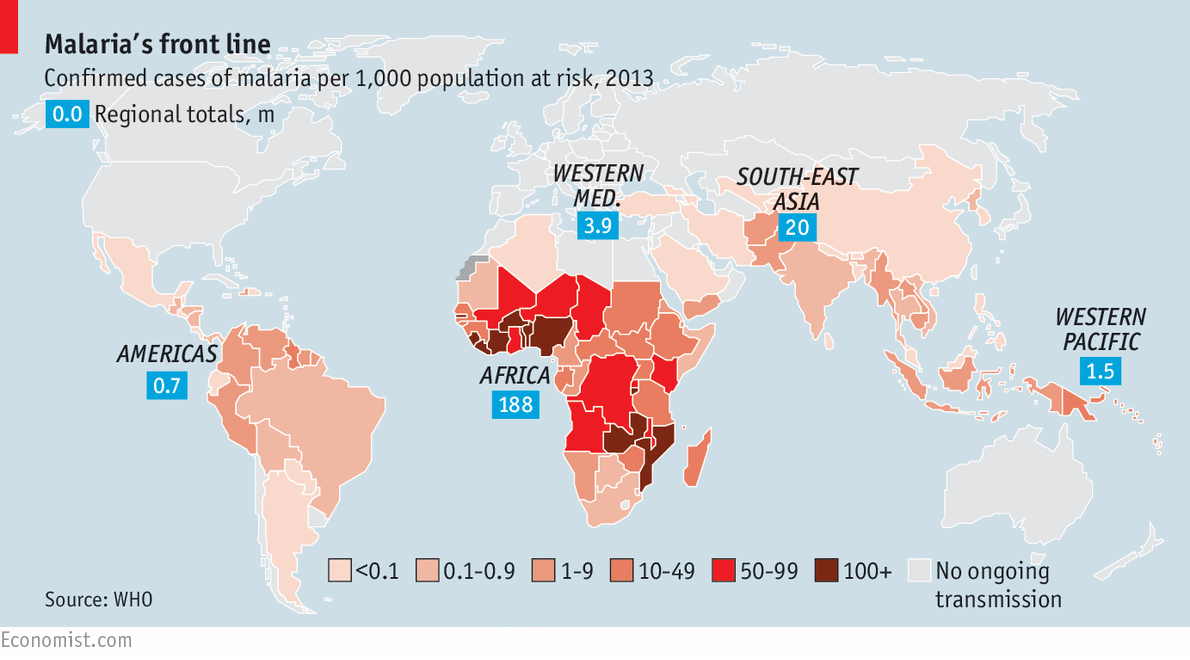
Since 2000, malaria deaths around the world have fallen by nearly half. The steepest drop has come in sub-Saharan Africa, where 90% of fatalities occur. Malaria still kills around 450,000 people each year (see chart 1)—most of them children in Africa. But the World Health Organisation (WHO) estimates that better control prevented the deaths of 3.9m African children between 2001 and 2013.

Such progress breeds optimism. The WHO believes that malaria cases and deaths could both fall by another 90% in the next 15 years. At a summit in November, heads of state from East Asia will endorse a plan to make the region free of malaria by 2030. The Gates Foundation, an important source of funds for antimalarial research and control efforts, believes it can be eradicated completely by 2040.
That would rank among humanity’s greatest achievements. Malaria has killed people since the dawn of man. In 1900 it was endemic in almost every country on Earth and throughout the first half of the 20th century it killed 2m people a year. Bringing malaria to heel has required not just money but also imagination, persistence and political will. Elimination would save millions of lives and trillions of dollars in lost productivity and health costs, mostly in poor countries.
Optimism, however, should be tempered by the recollection that past endeavours have failed. A global eradication effort begun in 1955 dramatically decreased malaria deaths over the following decade. But because of flaws in the programme, such as overreliance on too few drugs and a lack of adequately trained doctors, and because funding dried up as malaria cases fell, the disease came flying back. Laying the scourge to rest for good requires yesterday’s failures to inform today’s plans.
The disease starts with a bite from an infected mosquito, which injects a small number of parasites into its human victim’s bloodstream. Roughly 40 species of Anopheles mosquito, found all over the world, act as hosts for the types of malaria that affect humans. The parasites travel to the liver, where they multiply rapidly. They then infect red blood cells and continue to proliferate. Flu-like symptoms begin when the parasites break out of the blood cells, one to four weeks after the bite. Other mosquitoes can then pick up the parasite when they bite an infected person and pass it on when they bite another one.
Five types of malaria cause illness in humans. Plasmodium falciparum is responsible for the vast majority of deaths, having killed virtually all of the 528,000 people who died from malaria in sub-Saharan Africa in 2013. Plasmodium vivax is the most geographically widespread variety, responsible for most cases of malaria outside sub-Saharan Africa; it is less lethal than P. falciparum but can remain dormant in the liver and cause illness to recur when it emerges into the blood; frequent relapses weaken its victims, making them more susceptible to other diseases.
Eradication efforts focus on these two more virulent species. The other three strains usually cause less serious symptoms. But finding the victims and then stamping out mosquitoes and their deadly cargo of parasites is difficult. Up to 85% of people infected with malaria do not show symptoms and the parasite can lay dormant for months or years after an initial infection before emerging. This makes it especially tricky to fight.
The field tests that detect the parasite in places like Magagasi are not sensitive enough to pick up low-grade infections. Laboratory equipment that can detect the parasites is not available in every country. In Swaziland surveillance officers collect samples for laboratory analysis alongside rapid testing, and track them using bar codes and GPS co-ordinates to help them return to the right house. But no other African country has such a well-run system. Even so, finding Magagasi’s remaining carriers of the parasite has been a struggle. Laboratory tests take over a week to complete, which leaves plenty of time for mosquitoes to ferry the parasite to new victims.
Resistance is not futile
Taking on the malaria parasite and its insect hosts has proven equally hard. Both are frustratingly skilled at developing resistance to drugs or insecticides; and resistant strains tend to spread fast. In the early 20th century several countries reduced malaria by using DDT, a powerful insecticide, against Anopheles mosquitoes, until the insects developed resistance. Strains of P. falciparum resistant to chloroquine, once a common antimalarial drug, developed independently in several countries in the 1950s and 1960s; now they are everywhere.
Resistance works the other way, too. People who live in endemic areas become partially immune to the parasite as a result of repeated infections. Symptoms are most severe among children under five and become less serious as immunity builds over time, almost disappearing in some adults. Where malaria is eliminated, people lose immunity over time—so a recurrence of the disease can lead to an outbreak that affects everyone.
The front-line drug of choice, artemisinin-based combination therapies (ACTs), is used in most countries with P. falciparum and reduces malaria deaths in children by more than 96%. But artemisinin-resistant parasites have been found in five South-East Asian countries: Cambodia, Laos, Myanmar, Thailand and Vietnam. So far, most people with this type of parasite have recovered when treated with a combination of other drugs but some strains have proved resistant to almost all available antimalarial medications.
In Africa mosquitoes are rapidly developing resistance to the four insecticides that are used to treat bed nets and spray houses. Bed nets treated with insecticide are among the more effective and widespread low-cost measures. Most countries distribute them free. The share of the at-risk population sleeping under one rose from 3% in 2004 to 44% in 2013. But everywhere in Africa there are mosquitoes that have become resistant to pyrethroids, the chemicals used in two-thirds of house sprayings and the only type used to treat bed nets.
Resistance to two or more insecticides has developed in nearly two-thirds of malarial countries worldwide. If the high levels of resistance already seen in parts of western and southern Africa spread, then the most effective interventions of the past decade—bed nets and domestic insecticide treatments—could become ineffective.
The tenacity of malaria means that much more money will be required to wipe it out. For many years the research budget came from the military purse—particularly of Western armies that had to fight in tropical climates. Charities and governments of rich countries now pay for the fight against malaria. In recent years their contribution has grown dramatically, accounting for 82% of the $2.7 billion spent on control and elimination in 2013.
The largest single source is the Global Fund to Fight AIDS, TB and Malaria, which pools cash from developed countries, the private sector and charities. Between 2002 and 2013 the Global Fund spent $8 billion battling malaria. America also spends lavishly, both through donations to the Global Fund ($1.35 billion this fiscal year) and through other aid programmes, including the President’s Malaria Initiative, launched by George W. Bush in 2005 and now with an annual budget of $674m.
Even so, the Gates Foundation says that to remain on track to eradicate malaria, funding must double between now and 2025, when costs are expected to peak at $6 billion a year. The foundation puts the total cost of eradication at $90 billion-120 billion between now and 2040. Despite the steep price tag, the pay-off is far bigger: the Gates Foundation puts the total economic benefits of eradication from productivity gains and health savings in the same time period at more than $2 trillion.
As well as paying for current schemes, some of the cash goes to developing new weapons to ensure that malaria disappears for good. The armoury divides into three broad categories: new applications of existing treatments, novel treatments, and better diagnosis and surveillance.
In the first category, treating everyone in a village or region with antimalarial drugs can be effective. It tends to work best on settled populations, which may explain why its biggest success has been on a small island: Aneityum in Vanuatu. Nine rounds of mass drug treatment in 1991 helped eliminate malaria there. That lasted until 2002, when the disease was reintroduced, prompting another round of treatment that wiped it out again.
Myanmar has had some success, too—mass treatment of villages on the Thai-Myanmar border decreased the number of P. falciparum cases transmitted during the rainy seasons from 290 to 46 between 2011 and 2012—but without a better health system, mobile populations could well undo that success. More tests are under way in Asia and Africa on various drug combinations and on comparing their costs with other ways of eliminating malaria.
The second category of spending is on entirely new malaria treatments. Research-and-development spending on drugs, vaccines and basic research more than quadrupled between 1993 and 2013, reaching $550m annually.
Several candidates to supplement artemisinin are in the pipeline, but they will not be ready for release for many years. Nine additions to the array of insecticides are in development but none will be on the market for at least three years.
After decades of near misses, a vaccine is almost available. RTS,S (sic), the first to pass all stages of clinical trials, awaits WHO approval; European regulators nodded it through in July. Developed by GlaxoSmithKline, a drugs firm, and the Malaria Vaccine Initiative, an American non-profit organisation, RTS,S works, but not terribly well. It cuts the number of malaria episodes among infants and toddlers, typically one to five a year, by 36% over four years. It is not known how it will perform over a longer period.
That is about half the effectiveness needed for such a vaccine to become a potent weapon of eradication by greatly diluting the human reservoir of the parasite, says James Beeson of the Burnet Institute, an Australian research outfit. An ideal vaccine, says Mr Beeson, would have two components: one would stop infections in humans or stop infected humans from becoming sick; and the other would target transmission by making mosquitoes unable to pass on the malaria parasite. Separate vaccines for each of these tasks are in the pipeline but none is yet undergoing large-scale clinical trials.
Other approaches may prove more useful. Rather than attacking the parasite, another method is to modify its hosts. Researchers at Johns Hopkins University (JHU) in Baltimore have developed a genetically modified Anopheles mosquito that is highly resistant to the malaria parasite. Mating in the wild would pass this trait on to offspring, though mass release remains at least five years away. A new gene-editing technology called CRISPR would help malaria-resistant genes spread much faster through mosquito populations. It can enable a gene on one of the two chromosomes inherited by a mosquito to copy itself to the other, thus ensuring that all offspring inherit it.
Researchers are trying another technique in JHU’s giant greenhouse in Zambia: feeding mosquitoes sugar laced with a bacterium that blocks their ability to pass on malaria. A fungus with similar properties has also been discovered recently.
Better surveillance and diagnosis, the third front in the battle against malaria, have also helped bring down deaths. Diagnostic measures help with eradication for three reasons: people treated for malaria are less likely to develop the transmissible form of the parasite; correct diagnosis prevents overuse of antimalarials, thus slowing resistance; and better surveillance improves the aim of antimalarial activity by, say, giving priority to spraying and bed net distribution in areas with lots of confirmed cases of the disease.
In countries that have reached the elimination stage, defined by the WHO as those with less than one diagnosed case of malaria per 1,000 people at risk per year, strong surveillance systems are critical to prevent outbreaks. The WHO and the Cambodian government have trained a network of Village Malaria Workers—usually farmers or shop owners—to administer cheap, quick and reliable diagnostic tests to anyone suspected of having the disease. Such programmes reach people that national health systems cannot.
When someone with malaria shows up at a Swazi clinic, for instance, a nurse calls a national emergency number to report the case, which triggers an automatic text message to the phones of malaria-control programme managers. This helps them track the investigations of foot soldiers, who find out whether an infection occurred elsewhere and whether it has led to more cases.
Analysing information gathered on the ground in conjunction with other types of data can be used to direct interventions more accurately. Google and researchers at the University of California, San Francisco, have developed a prototype of a tool that uses weather, landscape and epidemiological-surveillance information to predict which villages are at high risk of malaria in certain months of the year—and should be first on the list for insecticide spraying and other preventive measures.
Better mapping could also help to track infections among mobile populations, who carry the malaria parasite across borders. Swaziland’s eradicators are busiest straight after Christmas, when the Mozambicans who work on the country’s sugar plantations return from visits across the border. Half Swaziland’s malaria cases are now imported.
In South-East Asia malaria spreads through areas with high shares of migrant workers. Systems to track it across borders are not yet in place. Botswana, Namibia, Swaziland and South Africa, which aim to eliminate malaria by 2020, are now setting up a regional co-ordination system with their northern neighbours that will include a joint reporting system, routine sharing of information on patterns of transmission in border regions and screening at border crossings.
The biggest challenge to eradication, however, is not mobile populations, the slow progress of vaccines or stiffening resistance, but the eradicators themselves. In the late 1960s, malaria rates had been brought close to zero in India, Pakistan, Haiti, Myanmar and dozens of other poor countries. But donors, governments and health systems declared victory too soon: their attention wandered, funding dried up and, over the next two decades, malaria came back.
Finishing the job
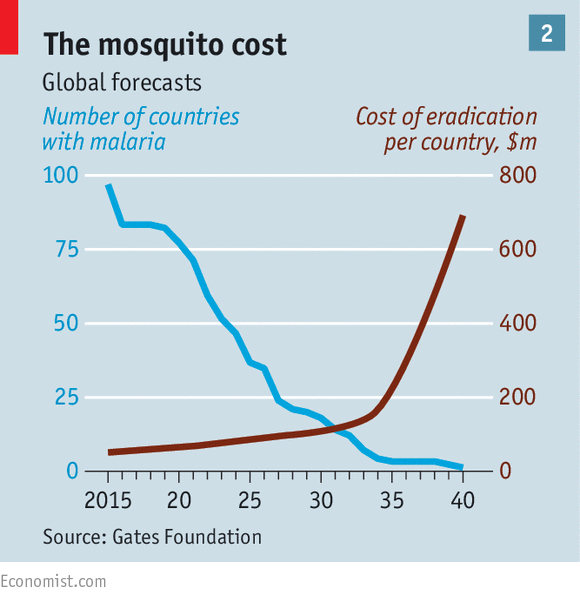
Today’s efforts are different. The drive of 50 years ago relied mainly on a single insecticide—DDT—and a single plan implemented across countries. Many therapies and interventions are now used and these are better integrated into national health systems. But as eradication efforts succeed, malaria risks dropping off the list of political priorities. As a growing number of countries eliminate malaria, eradication costs will fall overall but rise sharply in the remaining countries (see chart 2). These places, often war zones or failed states, tend to have a high prevalence of malaria and populations in remote and inaccessible areas, making eradication particularly costly. Funding needs to be maintained at sufficient levels and directed effectively to complete the task.
As it grows less prevalent, malaria moves from being a disease that can strike anyone to one that still afflicts the rural poor but that urban middle classes can ignore. Previous efforts to rid the world of malaria failed because the political will and funds dried up before the disease was conquered. This time it is vital that efforts to stamp out malaria do not become victims of their own success.
Be the first to comment