
Childhood obesity is reaching alarming proportions in many countries with 10.3 million African children under five years overweight or obese, according to a report by the World Health Organisation’s Commission on Ending Childhood Obesity.
The figure has almost doubled since 1990 (5.4 million) and accounts for 25 per cent of the 41 million children that were either overweight or obese globally in 2014.
This development, the report said, posed an urgent and serious challenge as obesity “has the potential to negate many of the health benefits that have contributed to increased life expectancy”.
The report, which noted that there were more overweight and obese children in middle-income countries than in high-income countries, stressed that obesity can affect a child’s immediate health, educational attainment and quality of life.
It added, “Children with obesity are very likely to remain obese as adults and are at risk of chronic illness.”
For instance it noted that obesity is a direct cause of diseases in childhood, including, sleep apnoea – a condition in which somebody stops breathing temporarily, especially while they are sleeping.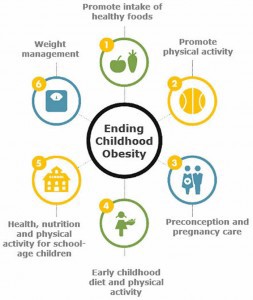
Others are injuries and diseases of the bones or muscles, stomach complications, type-2 diabetes and heart disease as well as the simultaneous presence of diabetes and heart disease.
Furthermore, it explained that obesity had physical and psychological health consequences during childhood, adolescence and into adulthood.
“Obesity in childhood can contribute to behavioural and emotional difficulties, such as depression, and can also lead to stigmatisation and poor socialisation and reduce educational attainment,” the report said.
Despite the risks, progress in tackling childhood obesity has been slow and inconsistent, according to the report.
It blamed the rise in obesity on poor nutrition and reduced physical activities, among other things, saying, “Many children today are growing up in an obesogenic environment that encourages weight gain and obesity.
“Energy imbalance has resulted from the changes in food type, availability, affordability and marketing, as well as a decline in physical activity, with more time being spent on screen-based and sedentary leisure activities.”
It explained that the behavioural and biological responses of a child to the obesogenic environment could be shaped by processes even before birth, placing an even greater number of children on the pathway to becoming obese when faced with an unhealthy diet and low physical activity.
It added, “Cultural values and norms influence the perception of healthy or desirable body weight, especially for infants, young children and women. In some settings, overweight and obesity are becoming social norms and thus contributing to the perpetuation of the obesogenic environment.”
The WHO Commission on Ending Childhood Obesity said tackling the growing obesity epidemic required the consideration of the environmental context and of three critical time periods in the life-course: preconception and pregnancy; infancy and early childhood; and older childhood and adolescence.
It added that the prevention and treatment of the problem required government support and buy-in.
Unfortunately, it said, “The greatest obstacle to effective progress on reducing childhood obesity is a lack of political commitment and a failure of governments and other actors to take ownership, leadership and necessary actions.”
Nevertheless, it called on governments to take leadership and for all stakeholders to recognise their moral responsibility in acting on behalf of the child to reduce the risk of obesity.
It also called for the implementation of comprehensive programmes that promote the intake of healthy foods and reduce the intake of unhealthy foods and sugar-sweetened beverages by children and adolescents.
Another recommendation was the implementation of comprehensive programmes that promote physical activity and reduce sedentary behaviours in children and adolescents.
The WHO urged governments and stakeholders to integrate and strengthen guidance for non-communicable disease prevention with current guidance for preconception and antenatal care, to reduce the risk of childhood obesity.
PUNCH
END
Be the first to comment